Wednesday 11 February 2015
God agrees with you, Stephen: the world was not meant to be this way
I love Stephen Fry. I went to see QI being filmed recently (the hardest I have laughed in a long time) and what struck me was that not only was he unbelievably funny but also very kind and gentle to the other panellists (except for the obligatory Aussie jokes about Colin Lane). I also have a huge amount of respect for how open he is about his struggles with depression. He is on my top ten list for “lunch and a chat” (not going to happen, I know).
Recently, though, Stephen has been making the news for his controversial comments about God. You can watch the clip here: https://www.youtube.com/watch?v=-suvkwNYSQo
For the record, I am really pleased that Stephen raised these points, even if his vehemence is a little startling at first (the interviewer certainly looks nonplussed). We need to talk about these things. Because there is a problem in our world, and it is a problem for which any worldview needs to have an explanation. It is the problem of suffering.
Now I am not a theologian; far wiser heads than mine will be able to give systematic Biblical answers to Stephen’s points. But I am a Christian, and one who has been through suffering personally, so needless to say I have grappled with these issues. I have been unwell fairly constantly for the last three years, and have experienced the ups and downs of chronic illness with periods of remission for all of my adult life. So Stephen’s comments took me back to the time when I had asked the same questions. It has been a long journey, and has taken an age of grappling, questioning and reading through the Bible for me to satisfy my intellectual and emotional conundrums about the problem of pain. It is something I still struggle with when a fresh set of symptoms appears.
When I was first admitted to hospital, acutely unwell with what was later diagnosed as a reactive arthritis, I felt like it was a slap in the face from a loving Father. I had trusted God since I was a child (deciding to follow Jesus at the age of three is one of my earliest memories). How could he turn round and do this to me? I learnt then that the people who say “your faith must be such a comfort to you in times of suffering” were sadly misguided; faith made it worse. If you believe in a personal God who loves you and is all powerful, what happens when you experience prolonged, intense suffering? Not only was I experiencing physical pain, but I was in the depths of emotional anguish. My worldview had been shaken.
If you are an atheist, there is no rhyme nor reason to suffering. Some people experience it, some people don’t, it’s pot luck. Stephen describes it as a “simpler” and “purer” existence. And lying there in my hospital bed, feeling like God had deserted me, I would have agreed with him.
The thoughts outlined below are the fruit of a long, hard struggle to come to terms with the way this world works and the way that the Bible talks about God. They put forward what I hope is a loving response to some of Stephen’s comments, based on the Bible and my own thoughts and struggles.
We cannot know everything about God.
It seems to me that a lot of Stephen’s frustration comes from the fact that he wants God to be quantifiable and all-knowable as well as all-knowing. This is a common human desire; to be able to tie everything up in a neat little package so that the world makes perfect sense in every minute detail as well as in the bigger picture.
Unfortunately, for God to be God, he has to be higher, bigger, mightier than us (otherwise he wouldn’t be God but would be some god we could keep in our pocket and trot out when it pleases us). In the book of Job, many questions about the purpose of suffering are asked and answered; some are left unanswered, which Job acknowledges at the end of the book: “Surely I spoke of things I did not understand, things too wonderful for me to know.” (Job 42:3).
We cannot understand everything about God, otherwise he would no longer be God. He has revealed himself to us in his word, the Bible, and through his Son Jesus coming to earth as a man. But there are still things that we don’t understand. In the same way that a child trusts her father to keep her safe and care for her, even when there are things about life she doesn’t understand, we are called to trust God as his children. And to be clear: when we see suffering in ourselves and others, that is really hard. I am not saying “trust God and suddenly all your questions will go away.” I am saying “there is one mightier in the universe than us, who has revealed himself to us as totally good and loving. When we have unanswered questions, we can hold to this truth and trust him, even when we have no clue about what’s going on.” It took me years to accept this, because it seems to be a cop-out answer. But trust is the key to any loving relationship, and the test of trust comes in hard times.
God did not make the world to be like this.
Stephen says to God “How dare you create a world in which there is such misery that’s not our fault? It’s not right. It’s utterly, utterly evil.”
God agrees with you Stephen: the world was not meant to be this way.
However, what we see now is not what was originally created. The beginning of the Bible says that God created everything and it was perfect and good. It was only when people broke their relationship with God that evil came into the world. We caused the pain and suffering that we see around us by believing that we know best and that God is a killjoy who wants to spoil our fun.
To be absolutely clear: I am not saying that individual people are at fault when they suffer in a kind of cosmic karma. I do not believe I am being punished for doing wrong when I experience daily pain; I do not believe that children with bone cancer that Stephen mentions are being punished for something they have done. Jesus makes this very clear in Luke’s account of his life (Luke 13:1-5).
“Now there were some present at that time who told Jesus about the Galileans whose blood Pilate had mixed with their sacrifices. Jesus answered, “Do you think that these Galileans were worse sinners than all the other Galileans because they suffered this way? I tell you, no! But unless you repent, you too will all perish. Or those eighteen who died when the tower in Siloam fell on them—do you think they were more guilty than all the others living in Jerusalem? I tell you, no! But unless you repent, you too will all perish.”
These people Jesus mentions are not “more guilty” than anyone else. We are not to think that they have done something especially bad which results in them being punished. But we are to look at these events and realise that there is something wrong with our world, and that we need to examine our own hearts and turn back to God (or repent, as the passage says) in light of these tragedies.
The Bible speaks of God being grieved by the suffering of the world and the evil of people (Genesis 6:5-7), of Jesus having compassion on those who are sick and bereaved (Luke 7: 11-17) and of God promising one day to make all things new, without sorrow or suffering (Revelation 21: 4-5). God agrees with you Stephen: the world was not meant to be like this, and he will one day fix the mess that we have made of it.
You cannot get angry about the suffering of the world without understanding the implications for your own heart.
It is very easy to point the finger at God. As Stephen says: “Yes the world is very splendid, but it also has insects whose whole life cycle is to burrow into the eyes of children and make them blind…why? Why did you do that to us? You could easily have made a creation in which that didn’t exist. It is simply not acceptable.”
When we look at the suffering of the world it is easy to point outside ourselves and say to God “Why don’t you come and sort this out?”
This is a question as old as the hills itself. It is a question I have repeatedly asked of God in the midst of weight loss, dehydration, unbearable pain, being unable to tie my shoelaces due to stiffness, fearing I might go blind, feeling that all my energy has been sapped so I can’t get out of bed in the morning, being unable to speak, unable to move my right arm and ultimately fearing that my body might just give out under all this pressure in the near future. It is no coincidence, then, that the book of Job, which deals almost entirely with the question of suffering, is the oldest book in the Bible. And in other parts of the Old Testament, we see God’s people asking similar questions:
“You have wearied the Lord with your words.
“How have we wearied him?” you ask.
By saying, “All who do evil are good in the eyes of the Lord, and he is pleased with them” or “Where is the God of justice?”” – Malachi 2: 17.
Sound familiar? The people of Malachi’s day were effectively saying “good is evil, evil is good, God doesn’t care and doesn’t do anything about it.” Unlike in the book of Job, their questions were asked out of a mixture of scorn and (perhaps) a small amount of desperation, as opposed to the anguished cry of a follower of God that we see in Job.
What is God’s response to the question “where is the God of justice”?
“"I will send my messenger, who will prepare the way before me. Then suddenly the Lord you are seeking will come to his temple; the messenger of the covenant, whom you desire, will come,” says the Lord Almighty. But who can endure the day of his coming? Who can stand when he appears? For he will be like a refiner’s fire or a launderer’s soap.” Malachi 3: 1-2.
God’s response is: I am coming. The God you are asking for will come and will make things right. But here’s the punchline: none of you can stand before him. No-one is pure, no one is fully right. No one is blameless. So if you are asking for God to come and put things right in this world, that has implications for you too, because none of us is without fault, and God has promised to come and purify his world and his people. The image of fire is not a comfortable one. God is not some cosy granddad – he is a totally pure and just God, and no one can stand before him and claim to be completely blameless.
God has come and done something about the evil and suffering in the world.
Stephen calls God capricious, a selfish maniac, evil, monstrous…the list of negative adjectives is seemingly endless.
Stephen’s description of God is based on his experience of the world around him. He looks at the world and sees all the suffering, and concludes that an all-powerful God who allows this suffering to continue must be evil and monstrous. Stephen’s logic is as follows:
1. The world was created as it is at the moment by God.
2. God claims to be all loving and all powerful.
3. The world as it is contains horrendous suffering.
4. Therefore God must be monstrous and capricious.
God’s answer? Well, God answered by showing up. Whatever else we think about the God of the Bible, we have to understand that the Bible says that God came to earth in the form of a man, suffered the most horrendous death on a cross, and was raised to life again three days later. The reason? As an example? As a political protest? No: he came to rescue us. Because within all of us there is evil which we need rescuing from. No one can stand the test of God’s perfect standards. Our relationship with the one who made everything good in the world is broken. That leaves us in trouble. But God has provided a way out, so that we can enjoy his favour and peace. He sacrificed his own Son to rescue us from the mess we had made for ourselves. As Paul says in Galatians 1: 3-5:
“Grace and peace to you from God our Father and the Lord Jesus Christ, who gave himself for our sins to rescue us from the present evil age, according to the will of our God and Father, to whom be glory for ever and ever. Amen.”
Does that sound like a selfish maniac to you? The giving of your only Son to rescue people who are in a mess entirely of their own making? It’s hardly the act of someone who is evil and monstrous. And whatever unanswered questions we have about the suffering in the world, the death of Jesus in our place stands as testament to God’s selfless, unfading love for those who have turned their back on him.
For me, believing in God and trusting in Jesus whilst daily experiencing chronic pain and ill health are not contradictory. The Bible engages with the questions of suffering, but does not give pat answers. I still have questions. But I know enough of God’s character, through the Bible and through my own personal experience of his daily provision, that I can say confidently that God is ultimately good and powerful. He did not intend the world to be like this. He has come to earth and died for us to demonstrate his love for us and to rescue us. He keeps me going through present hardships and uses them to bring about change in my own life and the lives of others. One day he will come back to make everything right. But all of this has implications for our own hearts, because none of us is totally blameless. We all need to think about how our worldview copes with the problem of pain. We all need to think about what we would actually say to a completely perfect and just God if he did come to earth to sort out the suffering and darkness in the world, including the darkness which lives in our own hearts.
And for the avoidance of doubt, I will still watch QI and laugh.
Tuesday 13 January 2015
My letter to NHS staff
There has been a lot in the news recently about pressures on the ambulance service, A&E and the NHS generally. In response to these headlines, personal stories have emerged of clinicians under pressure, with low morale and seemingly impossible demands on their already-stretched time.
I have a message for these clinicians, from paramedics to
porters, doctors to nurses, cleaners to receptionists, physios to SLTs – what I want to say as a patient applies to all
harried NHS workers. It comes out of my recent experience of two admissions to
A&E in quick succession this week, which allowed me to see first-hand the
pressures that staff are facing. I had outstanding treatment from some and
less-than-good treatment from others, and to be honest I am shocked that it
wasn’t all in the latter category, given what I observed in A&E; the
stories of people waiting in the corridors on trollies and slumped on chairs
have not been exaggerated. Here is my personal message for anyone who works in
the NHS.
Dear NHS workers,
I think I am finally beginning to understand. I had read the
news headlines (http://www.economist.com/news/britain/21638206-britains-national-health-services-accident-and-emergency-departments-are-under-renewed-pressure)
and I had read the personal stories (http://www.theguardian.com/society/guardianwitness-blog/2015/jan/08/surviving-night-nhs-hospital-a-and-e-doctors-story).
To be honest, none of it particularly surprised me. Having been in and out of
hospital for years and witnessed the chronic pressure placed on the NHS, I am
more surprised this hasn’t hit the headlines sooner. I am pretty sure that you,
working at the sharp end of things, have seen this storm brewing for a while.
This week I have had two episodes of unexplained aphasia
with neurological symptoms (muscle rigidity in my right arm). Both triggered
the stroke pathway when my friends phoned the ambulance service. What surprised
me was the time it took to get me to hospital on both occasions (around two hours
from when symptoms first hit). That doesn’t give the clinicians very long to
give clot-busting drugs within the four hour window in the event of a stroke.
But then it doesn’t surprise me, given that one of the ambulance men said he
had been called out to a 70 year old gentleman who complained of heavy,
crushing chest pain and breathlessness on the phone. When the paramedics got
there (within 7 minutes), it turned out he was fine; he just wanted someone to help him move his
TV. If paramedics are being called out to act as removal men, is it any wonder
that you guys are overstretched?
I want to say to you: I understand that you are short
staffed, overworked, underpaid, tired and stressed out and permanently
a little hypoglycaemic. That my condition (whatever it is) is not an open and
shut case, and that therefore it’s harder to be sympathetic because it takes
time to think about the right diagnostic tests and treatment. That it would be
easy to label me as faker number 11 when you’ve already had to deal with 10
such people today. But I am not faking. I am frightened. When the episode
strikes, I can’t speak. It’s not that I don’t want to. More than anything else,
I want to communicate and tell you what’s wrong. I know what I want to say, but
the words won’t come out. To those who have dismissed it as anxiety and told me
so to my face, I want to say: I get why you are saying this. It’s totally
understandable that you would want to make less work for yourself when you are
already hanging by your fingernails. But it doesn’t help: it adds fear and
anxiety to an already terrifying situation.
To those who have not dismissed me, I want to say: you are
heroes. To the doctor who came to take a case history when I could only say
nouns, and who allowed me the time to speak: wow. You probably had 30 other
patients clamouring for your attention, yet you gave me space and time without
jumping in and finishing my (very disjointed) sentences. And then when my speech returned, you
sat down with me for a good ten minutes and chatted with me about the Vikings.
I couldn’t work out what you were doing at first: were the reports of
overstretched staff greatly over-exaggerated, that you had ten whole minutes to
sit down and talk with me about something seemingly irrelevant? No, I realised
half-way through: you were doing a language sample, to check if my language had
indeed returned. You were making doubly sure I was recovered before you moved on.
To the nurse who took me down to CT and kept me chatting
whilst waiting for the scan; you were awesome company. I know I was a little
hyper after regaining my speech, and to be honest I can’t really remember everything
I said. I hope I didn’t embarrass you or say anything inappropriate, but to be
honest you were so kind that you would have taken it all in your stride.
To the paramedic called out on the weekend who initially
thought I was just overly anxious, then realised that there was probably more to
it than that and repeatedly apologised that the ambulance hadn’t come sooner
(and eventually took me to hospital in his fast response car): thank you for
changing your mind about me. I enjoyed your amusing stories about call-outs you’d
been on; they kept me calm and distracted from my fears.
To the nurse who confided in me about her long battle to get
a diagnosis for her endometriosis, and how she felt vindicated once she had
finally been told she wasn’t a morphine-seeker: thank you for confiding in me.
It made me feel that I wasn’t alone. Thank you for being blunt with me and
telling me “you are not crazy”. Thank you for telling me that you think it
could be migraines, and that this kind of migraine is becoming more common. I
felt so reassured that I wasn’t the only one experiencing this.
To the doctor who cleared up the blood I had spilt on the
floor after not putting pressure on my venepuncture site for long enough, and
for doing it with a wry smile – you didn’t have to do that. But thank you for
mucking in and helping, and not just leaving someone else to do it.
To the A&E junior doctor who spent a good half an hour
doing a thorough neurological exam: you did an excellent job. I know you had to
fight for that side room in which to do it, and that you had to turn porter for
a bit and find a bed to put me on, and wheel it down the corridor (I could tell
you weren’t very practiced at wheeling trolleys): that was beyond the call of
duty. Thank you for being humble and explaining that there are some things we
don’t understand about the brain and that we may not get the answer as to why
this is happening, but that this doesn’t mean what I am experiencing is not
real. Thank you for having the humility to admit you don’t know what’s going
on, and going off to chat to someone who knows more than you. Believe me, I
think more of you as a doctor for doing this, not less. Thank you for telling
me what to do next time this happens, and for ordering me to come in every time
I have an episode, even if I don’t want to bother the overburdened staff.
And to all the other staff who I didn’t interact with but
who made my stay in hospital marginally less stressful: the porters, cleaners,
receptionists, emergency department practitioners, CT scanner operators (are
you radiographers or radiologists? I can never remember): you are awesome. I
know you are tired, I know you are fed up with cumbersome targets. I don’t mind
if you don’t get me out of A&E within four hours (although you did: well
done!). I don’t mind if you bump me for someone who’s had a cardiac arrest, or
a child with suspected meningitis, or an elderly gentleman who has definitely
had a stroke / heart attack / fall; I can wait, their need is definitely
greater than mine. Just keep talking to me, keep listening to me, keep
remembering that this is a scary time for me, and that I wouldn’t be here
unless I needed your help. And once again: thank you.
Sunday 13 July 2014
I get it: but I'm still against assisted dying
As I sit here writing, my
back on fire, my feet feeling like they have shards of glass inserted deep into
the tendons, I want to say this: I get it. I have understood since I asked my
mum to remove the razors from my hospital bathroom. There is a desperation, a
hopelessness of facing a life where your current, terrible situation is
unlikely to improve that moves beyond depression into profound despair.
I am not pretending that I
understand (yet) what it is like to be in a wheelchair, though I sometimes need
to use sticks to walk. I am not pretending I know what it is like to be unable
to wipe my own bottom, though there are days when I can barely get off the
toilet and feel chained to it. I often have to make an unenviable choice
between passing the day in bone-deep, strength-sapping pain or taking pain
killers that dull the body and mind (not great when, as a PhD student, my
primary occupation is thinking). So no one can and should accuse me of not
understanding, of lacking compassion.
Because my fear is that this
is where the assisted dying debate is heading. In his recent article reversing
his opposition to assisted dying, former Archbishop of Canterbury Lord Carey
cites the need to prioritise "compassion" over "doctrine"
as being one of the key reasons for his change of stance (http://www.dailymail.co.uk/news/article-2689295/Carey-Ive-changed-mind-right-die-On-eve-Lords-debate-ex-Archbishop-dramatically-backs-assisted-death-law.html).
There seems to be a growing, insidious assertion by some promoting the assisted
dying bill that those in opposition are only against the bill because they
cling to outdated principles ("dogma", as Lord Carey calls it) and
place those principles above their compassion for fellow humans. "If only
you experienced or witnessed the suffering," the argument goes, "you
would surely change your mind."
This argument, whether made
overtly or covertly (and indeed deliberately or unconsciously) is deeply
patronising. "I am further down the road than you - if you had seen what I
have seen, experienced what I have experienced, you would come to the same
conclusions as I have."
To which I say: no. I live in
chronic pain, with little hope of long-term relief. I sometimes can't get off
the toilet. I have trouble walking. I sleep for ten hours a night and still
feel like I am wading through treacle. I know what it is like to suffer. Yet I
am against assisted dying, in spite of the fact that there are days when I
think: why go on? If this is it for the rest of your life, why continue?
My personal answers to those
questions are based heavily on my faith in a God who loves us and is in control
over what happens in our lives (a faith which, incidentally, is stronger now than
it has ever been, not in spite of but because of the suffering I am
experiencing). But even without such faith, there are strong arguments against
ending your life. And crucially, there are stronger arguments against changing
the law, which, we should not forget, is the primary issue which is currently
being debated in parliament.
The main reason, as the
current Archbishop of Canterbury Justin Welby has pointed out, is the precedent
that a change in the law would set, such that many elderly and vulnerable
people would feel duty-bound to end their lives (http://www.telegraph.co.uk/news/religion/10963362/Archbishop-Welby-Assisted-dying-is-sword-of-Damocles-over-vulnerable.html).
To those who dismiss this fear, I say this: I am a young and independent
person, yet I have sometimes fretted about the burden of worry and distress I
place on my loves ones, and thought in my darker moments that it may be better
for all concerned if I were to die and allow people to mourn and get on with
their lives. If this has crossed my mind, how much more so those who have
severe disabilities which place a great burden of care on their loved ones?
Up until now, premature death
has not been an option. But if this bill were to pass, it would open up the
possibility, which would be enough to cause great disquiet and distress in the
minds of countless people who feel themselves to be a burden. Lord Carey argues
that his change of stance is motivated by the desire to minimise anguish and
pain, in accordance with the Christian message of hope. What about the untold
anguish for countless numbers who would, if this bill were to pass, need to face the impossible decision of whether to end their own lives or continue living and being a burden on their loved ones? Surely this bill would compound
the distress of themselves and their family in an already difficult
situation? (For an excellent reflection on what this might look like, see Giles
Fraser’s blog: http://www.theguardian.com/commentisfree/belief/2014/jul/04/assisted-dying-triumph-market-capitalism)
The pro-assisted-dying argument
that counters the above assertion goes as follows: “this law would only apply
to a limited number of people, and strict safeguards would be put in place”. But
we can see from other countries such as the Netherlands that such laws rarely stay limited in this way (see the
comments of Dutch Professor Theo Boer, a former advocate of assisted dying: http://www.dailymail.co.uk/news/article-2686711/Dont-make-mistake-As-assisted-suicide-bill-goes-Lords-Dutch-regulator-backed-euthanasia-warns-Britain-leads-mass-killing.html)
“But why should people in
intolerable pain suffer for the sake of what might or might not happen further
down the road?” Let me flip this argument on its head: why should the many
disabled and vulnerable people who currently live in this country be put at
risk of harm and distress for the sake of a few, understandable though their
wish to die may be?
The quality of life argument
is also an interesting one. Lord Carey argues that it is quality of life, not
number of days, which is important. I agree. But poor quality of life is not
something set in stone; an impairment can be mitigated by societal and personal
factors. A person with chronic pain undoubtedly has reduced quality of life due
to their condition; however, the support of family and friends, the use of
medications and the development of new technological interventions can go some
way to counterbalancing this (see here for an awesome new invention designed to
help people who are paralysed: http://www.bbc.co.uk/news/health-27828553).
Poor quality of life is not a hopeless death sentence. Can we not focus on
improving people’s lives, rather than ending them?
I argue against assisted
dying in spite of my current state of chronic pain, for the sake of others who
cannot speak for themselves, and because ultimately all life is precious. You
may disagree with me. But please don’t say that I will only change my mind if I
could have experience of suffering. I have this in abundance.
Saturday 15 February 2014
A day in the life of a Crohnie
Happy New Year! (can I still say that on 15th February?) I guess when I haven't posted on my blog for a while, certain chronological liberties are permitted...
As many of you will know, I continue to battle with what has now been diagnosed as Crohn's disease. As well as new symptoms to cope with, I have noticed that there is a prevalent lack of awareness amongst the general population as to what Crohn's disease is, how it manifests, and how it can be treated.
So to combat this amongst my close friends and family (or at least amongst those of you who read this blog) I thought I'd set down, in all their glory, the main issues that I am currently experiencing, in an attempt to raise awareness of the impact of this disease. This post inevitably comes with a number of caveats:
1) The following information carries a TMI health warning (that stands for "too much information" for those of you not familiar with text-speak). I am going to detail what I experience on a daily basis, so the squeamish amongst you may not want to read further. Fair warning, but having said that, I make no apology for being honest about this debilitating disease, even if some of the symptoms do happen to be taboo. Maybe just don't read this over dinner...
2) My condition fluctuates, so what is detailed below is condensed information about the issues I experience. Perhaps "a month in the life of a Crohnie" would be a better title for this post, as I do not face all of these challenges every day (in case some of you were wondering how on earth I function with multiple awful symptoms).
3) I do not pretend to be representative of all people with Crohn's. Crohn's disease, perhaps more than most, is a highly variable condition in terms of its severity. I would say though that I am probably in the "moderate" category of disease severity, so that the burden of disease is about what an average person with Crohn's may face.
4) This is not meant to be a dig at friends or acquaintances for their ignorance! We've all been in that awkward situation where we've made a probably inappropriate comment and instantly regretted putting our foot in it with someone who is going through something alien from our own experiences. I just hope that by outlining the following challenges I can help you to understand better the experiences of people with inflammatory bowel disease in a non-accusatory or condemnatory tone.
So, having said all that, outlined below are the major challenges I am currently facing. If you have Crohn's or Ulcerative Colitis yourself, you may empathise with many of these, but feel free to post more in the comments section! And if you want to know more, please do ask. No question too awkward or gross (well, maybe).
1) Diarrhea. This is one the big symptoms of Crohn's. While I do not experience diarrhea every day, during a flare I can be going to the loo up to 15 times a day. Think back to the last time you had food poisoning (you really shouldn't have eaten that kebab from the roadside van, I mean, it's just common sense). Now imagine that instead of just a couple of days of diarrhea and pain, that was ongoing for weeks, and you'll have some idea of how exhausting the whole disease process is.
2) Fatigue. I guess this one is an obvious consequence from the first point. (I could make a joke here about number one and number two...oh wait, I just did). Fatigue is a direct consequence of the dehydration and weight loss caused by diarrhea, but is also compounded by the inflammatory processes that take place throughout the body (similar to what you experience when you have the flu).
3) Weight fluctuation. Before diagnosis, I lost 10% of my body weight, and am now close to regaining it and more due to the steroid medication I am taking to suppress disease activity. Unfortunately, the steroids cause your body to retain fat in rather odd places (most notably your cheeks, which results in the attractively termed "moon face" common in long-term users of oral steroids). Weight fluctuation is frustrating from a body image point of view, and practically means buying more clothes! Not that an excuse to buy more clothes is a particular tragedy for me...
4) Medication side-effects. Steroids cause a whole host of side-effects, but fortunately (perhaps) you can't be on them for too long. The longer-term medications such as azathioprine, however, are not much better. Drugs which suppress your immune system are likely to do so a little too well if you don't get the dose right, leaving you vulnerable to infections and bone marrow problems. Azathioprine is also classified as a carcenogenic substance, due to its association with an agressive form of lymphoma. It's difficult to put the tablet in your mouth and swallow it when you know all this!
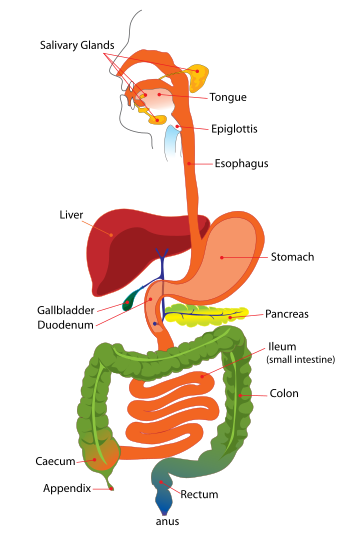
5) Malnutrition. My small bowel (see helpful multicoloured diagram if your anatomy is a bit fuzzy) seems to be one of the main offenders in this disease. This means that key nutrients such as calcium, iron and B12 (to name but a few) are not absorbed properly, no matter how much milk, spinach or marmite I ingest. Role on the B12 injections!
6) Arthritis. Many of you will know that I experienced the arthritis associated with IBD before the Crohn's symptoms became apparent. Unfortunately, most of the drugs used to control the arthritis pain (non-steroidal anti-inflammatories such as naproxen) cannot be taken by people with Crohn's due to the effect they have on the gut. Similarly, taking codeine is a bad idea as it causes constipation and accompanying gut pain and exacerbation of inflammation. So I am left with paracetamol and physio (30 minutes of exercises every morning for the rest of my life is a small price to pay for reduced pain and increased mobility!)
7) Uncertainty. While this is not really a symptom of Crohn's, it is a common feature of the disease. Everyone is individual, and every Crohnie's disease process is different. So it will take a while for me to work out what drugs work, how long they work for, and how severe my disease course will be. This causes a lot of anxiety and stress as I attempt to plan for the future without really knowing how debilitating the disease will be.
I think that's enough to be going on with. If you want to know more about the disease, please do visit the National Association for Crohn's and Colitis website: www.nacc.org.uk. I've just become a member so may be sporting some fetching red merchandise in weeks to come!
Thanks for reading :-) Hopefully this will have given you an insight into the "typical" challenges of someone with Crohn's and will help to raise awareness of this debilitating but often taboo disease.
Monday 23 December 2013
New Directions
The eagle-eyed amongst you will notice that my blog has changed. In place of a spine in the background, there is now a rather attractive image of the human digestive tract (believe me, there were plenty worse I could have chosen from!) Also, my strapline is different. This is because a new element has been added to my already complex health picture: Inflammatory Bowel Disease.
Most people, myself included, would never think to connect digestive system pathology with arthritis. The two conditions seem completely unrelated. In fact, how they are related is still something of a mystery, but what is known for sure is that approximately 20% of people with Inflammatory Bowel Disease also display some form of arthritis, which is often in the form of spondylitis (arthritis of the spine). There is a good summary of the condition to be found here:
http://www.healthline.com/health-slideshow/enteropathic-arthritis#1
My personal story is that recently I have been experiencing severe diarrhoea, abdominal pain and weight loss, which eventually culminated in an admission to the Royal London Hospital for a week in mid-December. Although the diagnosis is as yet unconfirmed, it is most likely to be Crohn's Disease, one of the two main types of IBD which can affect any part of the digestive tract. Mine appears to be in my small and large bowel, which as you might expect has caused a lot of difficulty in absorbing nutrients from food. The gastroenterologists have treated the inflammation aggressively with steroids, which appears to have helped; I am now waiting to hear as to the confirmation of the diagnosis and the extent of the inflammation via biopsies and scans undertaken during my time in hospital.
You might think that all of this is yet another blow to my health situation. It is indeed a lot to take in, and there are still many uncertainties with regards the disease extent and severity. But in fact, I had been warned by my rheumatologist in Bath that something like this might happen. He looked at my family history of Crohn's and the arthritis with which I presented to him and joined the dots correctly. I am almost looking forward to walking into my outpatient's appointment with him in January and telling him the news - it appeals to my Dr. House-like sense of diagnostic completion!
For now, this is a brief update post in between resting and Christmas festivities. In the future, I am hoping to write more on my blog about my experiences in hospital, living with IBD and the balancing act required to treat both Crohn's and the associated arthritis. For now, I would encourage you to read and learn more about IBD via the following website: www.nacc.org.uk. Perhaps due to British squeamishness about all-things toilet-related, IBD seems to me to be an under-recognised condition which is viewed as something of an embarrassment. I want to raise the profile of my newly-diagnosed condition and thereby hopefully help people understand what it is like to live with IBD, thus hopefully improving attitudes to those who suffer from Crohn's or Ulcerative Colitis.
But in the meantime, have a Wonderful Christmas! And don't eat too much :-)
Most people, myself included, would never think to connect digestive system pathology with arthritis. The two conditions seem completely unrelated. In fact, how they are related is still something of a mystery, but what is known for sure is that approximately 20% of people with Inflammatory Bowel Disease also display some form of arthritis, which is often in the form of spondylitis (arthritis of the spine). There is a good summary of the condition to be found here:
http://www.healthline.com/health-slideshow/enteropathic-arthritis#1
My personal story is that recently I have been experiencing severe diarrhoea, abdominal pain and weight loss, which eventually culminated in an admission to the Royal London Hospital for a week in mid-December. Although the diagnosis is as yet unconfirmed, it is most likely to be Crohn's Disease, one of the two main types of IBD which can affect any part of the digestive tract. Mine appears to be in my small and large bowel, which as you might expect has caused a lot of difficulty in absorbing nutrients from food. The gastroenterologists have treated the inflammation aggressively with steroids, which appears to have helped; I am now waiting to hear as to the confirmation of the diagnosis and the extent of the inflammation via biopsies and scans undertaken during my time in hospital.
You might think that all of this is yet another blow to my health situation. It is indeed a lot to take in, and there are still many uncertainties with regards the disease extent and severity. But in fact, I had been warned by my rheumatologist in Bath that something like this might happen. He looked at my family history of Crohn's and the arthritis with which I presented to him and joined the dots correctly. I am almost looking forward to walking into my outpatient's appointment with him in January and telling him the news - it appeals to my Dr. House-like sense of diagnostic completion!
For now, this is a brief update post in between resting and Christmas festivities. In the future, I am hoping to write more on my blog about my experiences in hospital, living with IBD and the balancing act required to treat both Crohn's and the associated arthritis. For now, I would encourage you to read and learn more about IBD via the following website: www.nacc.org.uk. Perhaps due to British squeamishness about all-things toilet-related, IBD seems to me to be an under-recognised condition which is viewed as something of an embarrassment. I want to raise the profile of my newly-diagnosed condition and thereby hopefully help people understand what it is like to live with IBD, thus hopefully improving attitudes to those who suffer from Crohn's or Ulcerative Colitis.
But in the meantime, have a Wonderful Christmas! And don't eat too much :-)
Tuesday 17 September 2013
Transport Dilemmas
Every year, like the inevitable turning of the leaves, darkening of the evenings and cooling of the temperature, comes the return of vast numbers of students to London after their summer break. This year, I was part of the mass Exodus, although my experience of the Autumn return has been somewhat different.
For a start, I did not simply go home to enjoy mum's cooking and Sky TV (though these were undoubted benefits). I went home partly to work in schools local to my parents' home, but also to recover having been newly diagnosed with spinal arthritis. My time at home was an ideal opportunity to develop good habits in terms of physiotherapy and pacing in preparation for return to the frenetic London life.
And it is frenetic. I don't think I'd realised before how physically and mentally draining it is to live here, and dealing with a chronic condition only accentuates this. It has been since coming back to London and comparing life here with life at home that I have come to realise this stark contrast. So here are some of my reflections. They form part of a wider series of posts that I hope to be writing in the coming months, outlining everyday dilemmas that people with chronic conditions face. Some of them may seem trivial, but they have been my constant companions recently and so I thought it would be useful to reflect on some of them.
This post will focus on transport. Now Londoners are never shy of complaining about the tube / buses / cars / cyclists / whatever other mode of transport happens to be subject to their disapproving scrutiny. But there are difficulties with transport that a traveller can face beyond the hazards of signal failures and leaves on the line (which would be impressive on the underground).
1) My transport dilemmas begin before I leave the house. The first question is: do I walk to the station nearby or do I get a bus from outside the door to a different station? Both have their positives and negatives. Walking is good for my back, but bad for my knees, especially on hard London pavements. Walking is also quicker (strangely) as I use a route which gets me to work faster than the bus option. I have to weigh up whether my knees will last the 10-minute walk given their recent grumbling / the weight of my rucksack / the speed at which I need to walk in order to be on time.
2) Do I take my sticks? You might think it was an easy decision based purely on whether I need them to walk. Not so. Because depending on the time at which I wish to travel, I may not get a seat without them. So if I do not take them and then don't get a seat, I will paradoxically be more likely to need them to support me when I'm standing on the rocking train. Unlike those with a "baby on board", I do not have the convenience of being able to pin an "unseen disability" badge to my coat.
3) If I don't take my sticks and do manage to get a seat, do I give the seat up to the elderly woman who is forced to stand by the stubbornly oblivious passengers who bury themselves in their newspapers? Is her need greater than mine? How do I tell? What does she think of a young person taking a seat when she has to stand? I have not had many experiences of being reprimanded for taking the priority seat, but they have happened (and one of them was when I had crutches on prominent display).
4) Would it be better to call the whole thing off and take a taxi? I have thankfully been provided with a taxi fund by the Disabled Students' Allowance this year, but this comes with certain conditions. I have to pay a student contribution on the grounds that all students pay for travel costs (even though normally I travel on a travelcard, so this works out as an extra cost for me). The taxi service, however, is not particularly reliable, and the nature of my work is such that I do not always know when I will need to travel (and the taxis have to be booked in advance). So then I can end up standing around waiting when all I want to do is go home and rest, and when it would be quicker (and cheaper) to take public transport.
The solution? I'm still working on that one. Sometimes I address these dilemmas and make choices that may be good or bad ones with hindsight. At other times, I work from home. The joys of being a PhD student.
For a start, I did not simply go home to enjoy mum's cooking and Sky TV (though these were undoubted benefits). I went home partly to work in schools local to my parents' home, but also to recover having been newly diagnosed with spinal arthritis. My time at home was an ideal opportunity to develop good habits in terms of physiotherapy and pacing in preparation for return to the frenetic London life.
And it is frenetic. I don't think I'd realised before how physically and mentally draining it is to live here, and dealing with a chronic condition only accentuates this. It has been since coming back to London and comparing life here with life at home that I have come to realise this stark contrast. So here are some of my reflections. They form part of a wider series of posts that I hope to be writing in the coming months, outlining everyday dilemmas that people with chronic conditions face. Some of them may seem trivial, but they have been my constant companions recently and so I thought it would be useful to reflect on some of them.
This post will focus on transport. Now Londoners are never shy of complaining about the tube / buses / cars / cyclists / whatever other mode of transport happens to be subject to their disapproving scrutiny. But there are difficulties with transport that a traveller can face beyond the hazards of signal failures and leaves on the line (which would be impressive on the underground).
1) My transport dilemmas begin before I leave the house. The first question is: do I walk to the station nearby or do I get a bus from outside the door to a different station? Both have their positives and negatives. Walking is good for my back, but bad for my knees, especially on hard London pavements. Walking is also quicker (strangely) as I use a route which gets me to work faster than the bus option. I have to weigh up whether my knees will last the 10-minute walk given their recent grumbling / the weight of my rucksack / the speed at which I need to walk in order to be on time.
2) Do I take my sticks? You might think it was an easy decision based purely on whether I need them to walk. Not so. Because depending on the time at which I wish to travel, I may not get a seat without them. So if I do not take them and then don't get a seat, I will paradoxically be more likely to need them to support me when I'm standing on the rocking train. Unlike those with a "baby on board", I do not have the convenience of being able to pin an "unseen disability" badge to my coat.
3) If I don't take my sticks and do manage to get a seat, do I give the seat up to the elderly woman who is forced to stand by the stubbornly oblivious passengers who bury themselves in their newspapers? Is her need greater than mine? How do I tell? What does she think of a young person taking a seat when she has to stand? I have not had many experiences of being reprimanded for taking the priority seat, but they have happened (and one of them was when I had crutches on prominent display).
4) Would it be better to call the whole thing off and take a taxi? I have thankfully been provided with a taxi fund by the Disabled Students' Allowance this year, but this comes with certain conditions. I have to pay a student contribution on the grounds that all students pay for travel costs (even though normally I travel on a travelcard, so this works out as an extra cost for me). The taxi service, however, is not particularly reliable, and the nature of my work is such that I do not always know when I will need to travel (and the taxis have to be booked in advance). So then I can end up standing around waiting when all I want to do is go home and rest, and when it would be quicker (and cheaper) to take public transport.
The solution? I'm still working on that one. Sometimes I address these dilemmas and make choices that may be good or bad ones with hindsight. At other times, I work from home. The joys of being a PhD student.
Saturday 27 July 2013
Daily life
It's been a while since I've posted here, mostly because PhD-related matters have taken over, so that I have become obsessed with p-values as a way of validating the last 12 weeks of my life and work (thankfully I can say I have reached the magic value of p<0.05, so all is well).
I thought that I'd use my return to the world of blogging as a way of revisiting my original purpose for writing this blog; to be a helpful and insightful source of information about everyday life living with a chronic condition.
I want to write about this because I strongly believe that, as a society, we are not well-equipped for dealing with people with chronic conditions (that is, conditions that are not life-threatening, but from which a patient never truly recovers).
You can see hints of this in your local stationery shop. What choice of message do you really have when trying to find a card for someone who's unwell? It essentially boils down to "Get well soon" cards. The imperative nature of this sentence implies a command rather than a hope, and therefore that getting well is somehow in the patient's control (who would love to be better in a flash, but unfortunately life doesn't work like that). These cards reflect the fact that in our society, it seems, there are broadly two categories of people:
1) Those who are acutely ill, who spend their time of sickness in a hospital (rather than in days gone by, when the ill and infirm would often have been cared for at home). The unwell are encouraged to "get well soon" as quickly as possible so they can rejoin group number 2.
2) The completely well, who are able to run around and take part in every single activity that today's frenetic lifestyle throws at them.
It is as if we've forgotten that there are people out there in our homes, schools, places of work, on the bus, attending outpatient appointments, who in fact live every day with some reminder of their chronic condition. And I believe we often forget because those of us with chronic conditions feel a lot of pressure (from within ourselves as well as out there in society) to hide the condition that we live with.
Let me illustrate this with another example. I am often greeted by friends who haven't seen me for a while with "You're looking much better" or "Are you feeling any better?" (please don't worry if you can remember saying this to me at some point - I am as guilty of it as the next person, and I have even less excuse!) Do you see what this does to the listener? Like the ever-more-ubiquitous "how are you?", we are forced to reply yes or agree with the assessment that things are looking up.
Of course, everyone would love it (me most of all) if I could permanently ditch my sticks. But sadly, chronic conditions do not work like that. And by implying, however subtly, that the person in front of you "really should be better by now", you can inadvertently make someone feel guilty for their illness (I would think this is particularly true of people with long-term depression or other mental health conditions, though I have less direct experience of this).
So I would encourage you to remember that there is indeed a group number 3) to add to my analysis above. They are people who live daily life with permanent reminders of a chronic conditions, whether through taking pills, struggling with fatigue, experiencing mental highs and lows, or grappling with unrelenting pain. They are all around you, and many of them will hide their illness or disability in an effort to keep up with today's hectic lifestyle.
How about asking them "So how's life really going for you?" as a way to unlock how things are really going for them? You might be surprised, both by how difficult daily life is for them, and how grateful they are that you've taken an interest.
I thought that I'd use my return to the world of blogging as a way of revisiting my original purpose for writing this blog; to be a helpful and insightful source of information about everyday life living with a chronic condition.
I want to write about this because I strongly believe that, as a society, we are not well-equipped for dealing with people with chronic conditions (that is, conditions that are not life-threatening, but from which a patient never truly recovers).
You can see hints of this in your local stationery shop. What choice of message do you really have when trying to find a card for someone who's unwell? It essentially boils down to "Get well soon" cards. The imperative nature of this sentence implies a command rather than a hope, and therefore that getting well is somehow in the patient's control (who would love to be better in a flash, but unfortunately life doesn't work like that). These cards reflect the fact that in our society, it seems, there are broadly two categories of people:
1) Those who are acutely ill, who spend their time of sickness in a hospital (rather than in days gone by, when the ill and infirm would often have been cared for at home). The unwell are encouraged to "get well soon" as quickly as possible so they can rejoin group number 2.
2) The completely well, who are able to run around and take part in every single activity that today's frenetic lifestyle throws at them.
It is as if we've forgotten that there are people out there in our homes, schools, places of work, on the bus, attending outpatient appointments, who in fact live every day with some reminder of their chronic condition. And I believe we often forget because those of us with chronic conditions feel a lot of pressure (from within ourselves as well as out there in society) to hide the condition that we live with.
Let me illustrate this with another example. I am often greeted by friends who haven't seen me for a while with "You're looking much better" or "Are you feeling any better?" (please don't worry if you can remember saying this to me at some point - I am as guilty of it as the next person, and I have even less excuse!) Do you see what this does to the listener? Like the ever-more-ubiquitous "how are you?", we are forced to reply yes or agree with the assessment that things are looking up.
Of course, everyone would love it (me most of all) if I could permanently ditch my sticks. But sadly, chronic conditions do not work like that. And by implying, however subtly, that the person in front of you "really should be better by now", you can inadvertently make someone feel guilty for their illness (I would think this is particularly true of people with long-term depression or other mental health conditions, though I have less direct experience of this).
So I would encourage you to remember that there is indeed a group number 3) to add to my analysis above. They are people who live daily life with permanent reminders of a chronic conditions, whether through taking pills, struggling with fatigue, experiencing mental highs and lows, or grappling with unrelenting pain. They are all around you, and many of them will hide their illness or disability in an effort to keep up with today's hectic lifestyle.
How about asking them "So how's life really going for you?" as a way to unlock how things are really going for them? You might be surprised, both by how difficult daily life is for them, and how grateful they are that you've taken an interest.
Subscribe to:
Posts (Atom)